
Case Report: Acute Monocular Painless Vision Loss in Elderly Man
A 79-year-old male with a history of diabetes mellitus, atrial fibrillation, and hyperlipidemia presented to the Emergency Department (ED) with a chief complaint of painless left eye vision loss. His symptoms started the previous night, approximately 20 hours prior to arrival, and were described as a sudden onset of “cloudy and darkening” vision from his left eye, which rapidly progressed to complete vision loss within minutes. Vision from his right eye remained unchanged. He noted that he had a history of uncomplicated cataract surgery to his left eye four months prior, and his family noted that he had stopped taking Xarelto one month ago. The patient otherwise denied other symptoms.
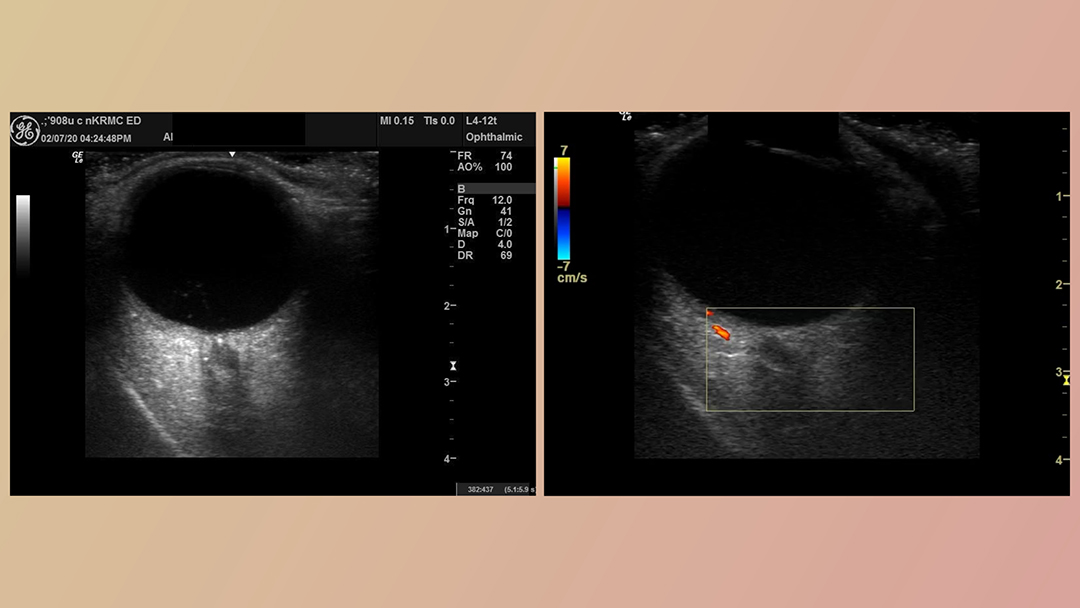
During his initial presentation, his vital signs were within normal limits. On physical examination, he was noted to have an afferent pupillary defect as well as significantly reduced visual acuity in the left eye (20/200). Intraocular pressures were 14 mmHg and 11 mmHg in the left and right eyes, respectively. Ocular point-of-care-ultrasound (POCUS) was performed using a 12 Megahertz (MHz) linear probe (Fig. 1).
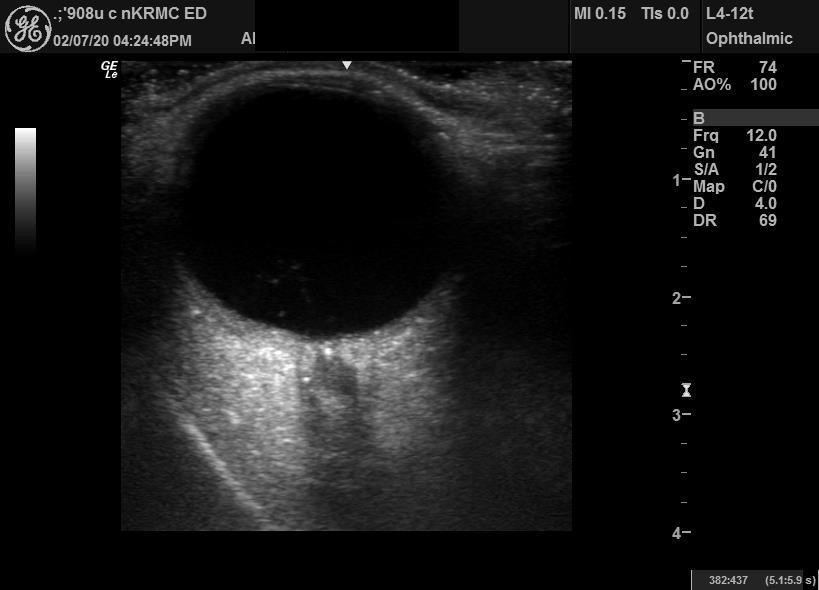
Fig. 1 – Ultrasonography of the left eye obtained with the linear probe in axial-transverse axis with the patient in the supine position, demonstrating a retrobulbar hyperechoic focus (retrobulbar spot sign) at the junction of the optic nerve and the globe, highly suggestive of emboli.
Diagnosis: Central Retinal Artery Occlusion (CRAO)
CRAO is classically diagnosed in patients presenting with painless vision loss via fundoscopy, demonstrating a pale retina with a “cherry red” spot, retinal edema, and narrowing of blood vessels. This constellation of signs signifies ischemia of the main arteries supplying blood to the retina. Visualization of the retinal vasculature via fundoscopy is frequently difficult and limited without a dilated eye examination. Furthermore, as demonstrated by a prior study, the visualization of the thrombi in patients with CRAO view fundoscopy is only accomplished in 11% of patients (1). The utilization of point-of-care ultrasound can aid in the differentiation of CRAO from other causes of acute painless vision loss (2).
The central retinal artery, arising from the ophthalmic artery (first branch of the internal carotid artery), travels within the optic nerve upon entering the orbit and enters the eye. A retrobulbar spot sign was present in this case, demonstrating the utility of POCUS in being able to rapidly identify the thrombus within the central retinal artery, leading to the visual diagnosis of CRAO without fundoscopy. In a study of 31 patients with CRAO, 59% were found to have a retrobulbar spot sign, supporting the utility of bedside ultrasonography for this diagnosis (3). Given the diagnostic inaccuracy of bedside fundoscopy, these studies indicate the POCUS could be a powerful tool to expedite the diagnosis of this entity.
Our patient had no other signs of retinal detachment, vitreous detachment, or vitreous hemorrhage noted. The diagnosis of CRAO was confirmed by dilated eye examination by the consulted ophthalmologist. He was subsequently found to have high-grade bilateral carotid bifurcation plaque formation and stenosis. He eventually underwent bilateral carotid endarterectomy.
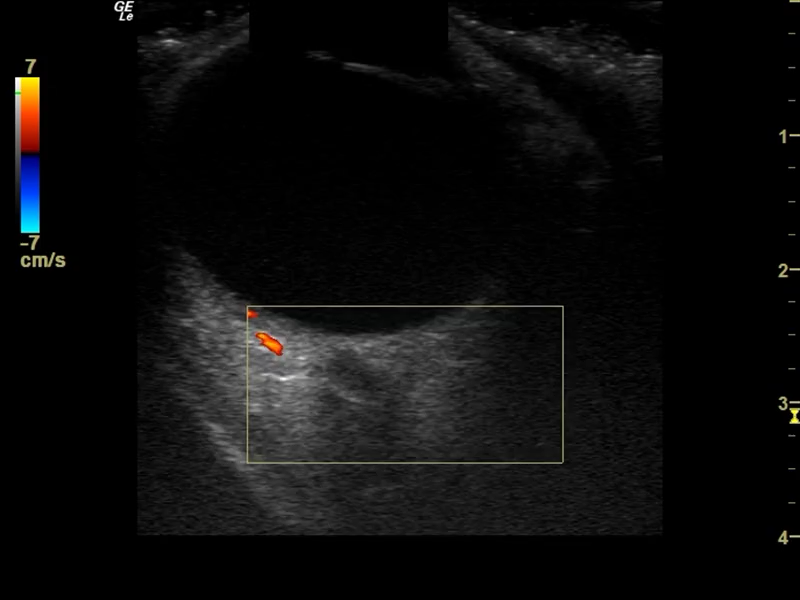
Fig. 2 – Application of Color Doppler to optic disc demonstrates absence of vascular perfusion.

References:
- Schmidt D, Hetzel A, Geibel-Zehender A, Schulte-Mönting. Systemic diseases in non-inflammatory branch and central retinal artery occlusion–an overview of 416 patients. 2007 Dec 14, Eur J Med Res, pp. 12(12):595-603. PMID: 18024271.
- Ertl M, Altmann M, Torka E, Helbig H, Bogdahn U, Gamulescu A, Schlachetzki F. The retrobulbar “spot sign” as a discriminator between vasculitic and thrombo-embolic affections of the retinal blood supply. ltraschall Med. 2012 Dec;33(7):E263-E267. doi: 10. Ultraschall Med., 2012 Dec, Vols. 33(7):E263-E267. doi: 10.
- Rudkin AK, Lee AW, Chen CS. Vascular risk factors for central retinal artery occlusion. London: Eye (Lond)., 2010 Apr, Vols. 24(4):678-81. doi: 10.1038/eye.2009.142. Epub 2009 Jun 12. PMID: 19521436.
This article is part of the following sections:




{kind=link}