

Left Lateral Canthotomy with Cantholysis for Foreign Body Removal in the Emergency Department
Introduction
Lateral canthotomy and cantholysis is a vision-saving procedure most commonly used to relieve orbital compartment syndrome caused by retrobulbar hemorrhage, usually secondary to facial trauma. Bleeding in the enclosed bony orbit causes increased intraorbital pressure and resultant ischemia of the retina and optic nerve, leading to rapid and irreversible blindness. [1,2,3]
Despite its importance, lateral canthotomy and cantholysis is not often performed in the emergency department due to the rarity of the specific pathology requiring the procedure. The reported incidence of retrobulbar hematoma after blunt facial trauma is less than 1%, limiting a physician’s opportunity to perform the procedure. [3]
The use and utility of lateral canthotomy and cantholysis in the emergency department for conditions other than orbital compartment syndrome are underreported. A case is presented involving the use of lateral canthotomy and cantholysis for orbital foreign body removal.
Case Presentation
A 51-year-old male presented to the emergency department for evaluation of a left-eye foreign body.
One hour prior to arrival, the patient was trimming a palm tree when a palm frond fell and knocked off his safety goggles. The patient felt a thorn enter his left eye. He complained of discomfort in the eye but denied any vision changes.
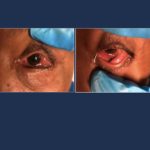
On exam, visual acuity was 20/100 in the right eye and 20/400 in the left eye. The pupils were equal, round, and reactive to light and accommodation. Extraocular movement and confrontational visual field testing were limited in the left eye secondary to pain. The left conjunctiva was injected with chemosis (Fig. 1). On Wood’s lamp examination, there was no Seidel sign and no fluorescein uptake.
Tonometry measurement was deferred due to the presence of a foreign body. A linear foreign body was embedded into the inferior conjunctival fornix directed from the inferomedial orbit to the temporal orbit (Fig. 2).
Decision Making
An attempt was made to remove the foreign body using forceps. The attempt was aborted when it was discovered that the foreign body penetrated deeper than initially believed and the risk of foreign body fracture or splintering was identified. Ophthalmology was consulted and arrived at the bedside to further manage the patient. The inferomedial portion was freed from the inferior conjunctiva (Fig. 3). At this point, concern arose over potential globe rupture and a CT of the orbits was obtained (Fig. 4). The CT revealed no globe penetration and the decision was made to perform a lateral canthotomy and cantholysis to facilitate the foreign body removal.
Lateral canthotomy and cantholysis is a rarely-performed, vision-saving procedure. [4] The primary indications for performing the procedure are suspicion of orbital compartment syndrome with at least one of the following: decreased visual acuity, intraocular pressure > 40 mm Hg, and proptosis. Secondary indications include: afferent pupillary defect; cherry red macula; ophthalmoplegia; nerve head pallor; and eye pain. [5]
The patient in this case lacked any of the primary indications listed, though it is important to note that intraocular pressure was not measured. On initial exam, the foreign body appeared to be much shorter than its true length. This highlights the importance to consider a more complex injury when managing any ocular or orbital trauma.

Fig. 1. Injected conjunctiva with chemosis

Fig. 2. Foreign body embedded into the inferior conjunctival fornix

Fig. 3. Release of the inferomedial portion of the foreign body

Fig. 4. 2 cm linear low-density foreign body without globe involvement
As the use of lateral canthotomy and cantholysis for foreign body removal in the emergency department is underreported, more research is needed to study the benefits and risks of performing the procedure without a primary indication. This case is one example of the utility of the procedure for a non-indicated condition.
Conclusion
Patients who present to the emergency department for evaluation of orbital foreign bodies should be screened for globe rupture or penetration. Those with complex lateral conjunctival foreign body embedment without globe injury should be considered candidates for lateral canthotomy and cantholysis. ■
REFERENCES
- Rixen J, Randall Verdick BA, Allen RC, Carter KD. Lateral canthotomy, inferior cantholysis. The University of Iowa Department of Ophthalmology and Visual Sciences EyeRounds Website. 2013 Mar 12 [accessed 2021 Aug 23]. webeye.ophth.uiowa.edu/eyeforum/tutorials/lateral-canthotomy-cantholysis.htm
- Desai NM, Shah Su. Lateral Orbital Canthotomy. [Updated 2021 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan. Available from: ncbi.nlm.nih.gov/books/NBK557476/
- Fattahi T, Brewer K, Retana A, Ogledzki M. Incidence of retrobulbar hemorrhage in the emergency department. Journal of oral and maxillofacial surgery: official journal of the American Association of Oral and Maxillofacial Surgeons. 2014;72(12):2500–2502.
- Rowh AD, Ufberg JW, Chan TC, Vilke GM, Harrigan RA. Lateral canthotomy and cantholysis: emergency management of orbital compartment syndrome. The Journal of emergency medicine. 2015;48(3):325–330.
- McInnes G, Howes DW. Lateral canthotomy and cantholysis: a simple, vision-saving procedure. CJEM. 2002;4(01):49–52.
This article is part of the following sections:
Rolando Zamora Jr., MD

Joseph J. Gomes, DO

Iris C. Cruz, APRN
-
Iris C. Cruz, APRN#molongui-disabled-link



{kind=link}