
Summer 2020: Daunting Diagnosis
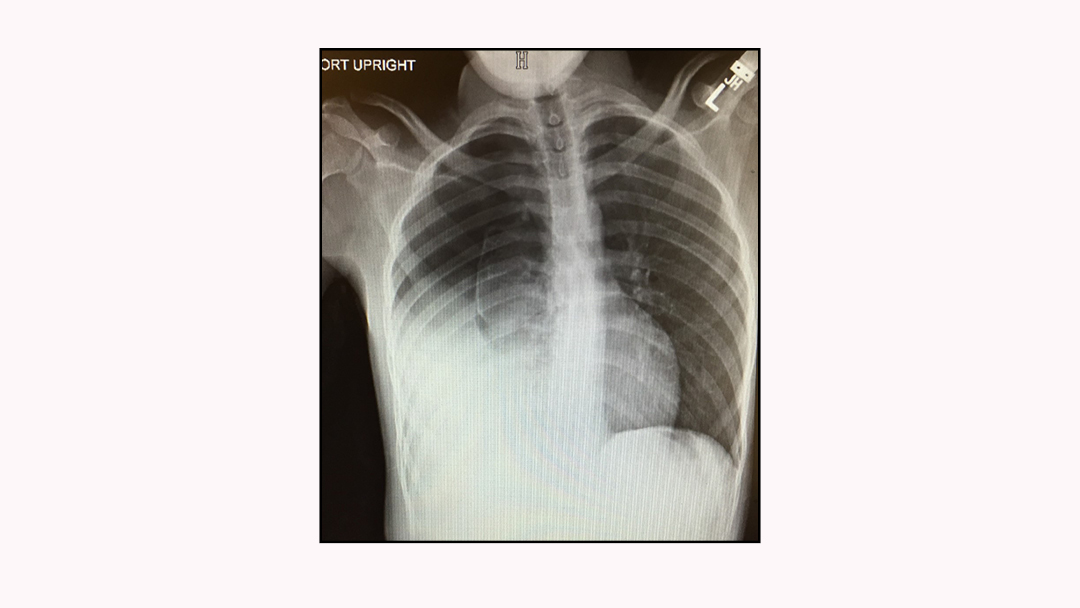
A 19-year-old autistic male presents to the ED with his parents for right upper back pain. The patient is a poor historian, and the parents are unable to give any definitive history. There is no recollection of trauma, no obvious musculoskeletal injury, and no cough. Vitals are remarkable for a heart rate of 144 and respirations of 26. The patient is afebrile. The mother attributes his tachycardia to anxiety, stating the patient is often highly anxious. What does the radiograph show?

Answer:
The chest XR was initially read by the radiologist as a “hydrothorax.” To further evaluate the hydrothorax, a rapid chest CT was obtained while the patient was set up for a chest tube insertion under conscious sedation.
Upon insertion of a right-sided chest tube, over 1000cc of bright red blood was evacuated from the chest cavity. Heart rate improved to the 120’s, and the patient was admitted to the SICU under cardiothoracic surgery.
Throughout the week, chest tube drainage was monitored by the SICU team. The chest tube was eventually removed, and the patient was discharged home with no further insight into why he accumulated a massive hemothorax.
One week later, the patient presented again to the ED with fever, tachycardia, and tachypnea.
The patient now presents with sepsis from an empyema. A sepsis protocol was initiated, and the patient was admitted to cardiothoracic surgery for urgent pleurodesis. The patient tolerated surgery well, although his disease pathogenesis still remains a mystery. ■



This article is part of the following sections:
 This article originally appeared in EMpulse Summer 2020. View the full print version of the magazine here.
This article originally appeared in EMpulse Summer 2020. View the full print version of the magazine here.



{kind=link}